



Do You Need a Measles Vaccine?
March 21, 2025
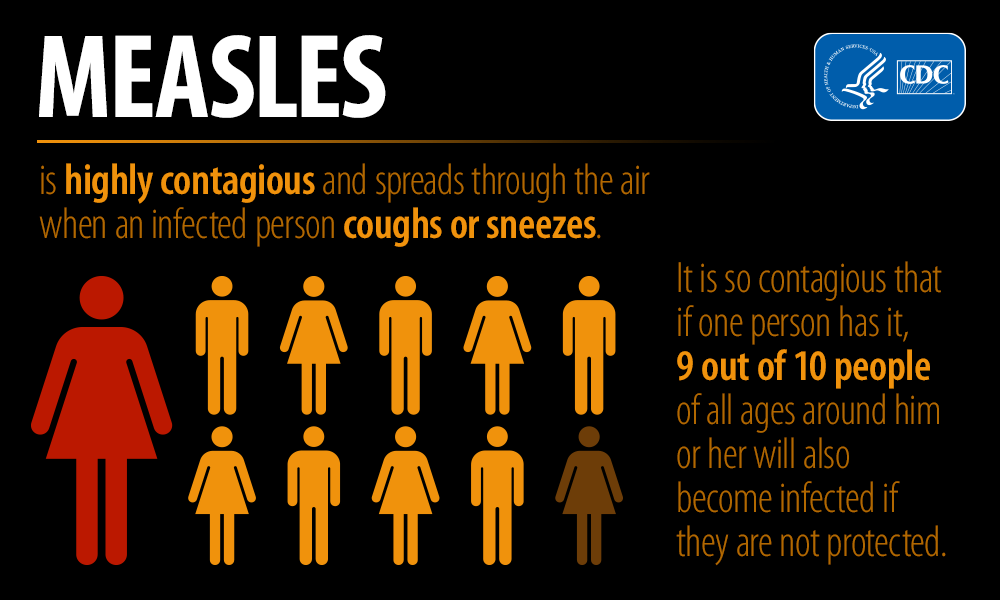
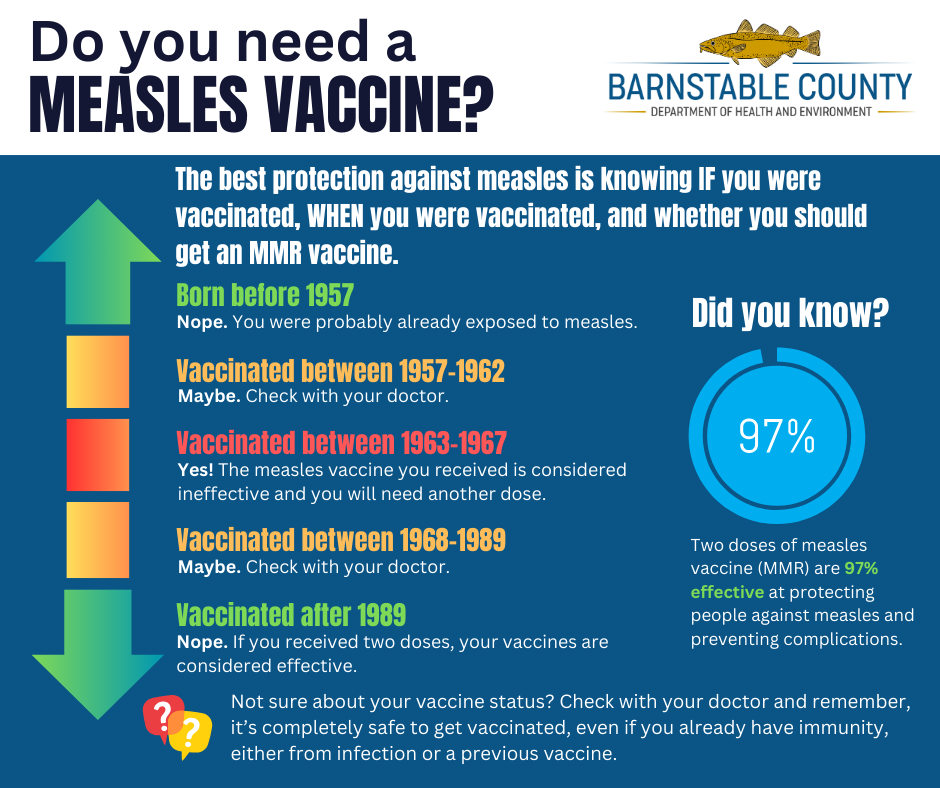
The best protection against measles is knowing IF you were vaccinated, WHEN you were vaccinated, and whether you should get a Measles, Mumps, & Rubella (MMR) vaccine. Most people who […]
Read More